A little late getting today’s post up, but here it is. In several recent posts I’ve alluded to surgery that I’m going to have soon, but haven’t given specific info. It will be open-heart surgery.
Now, before everyone freaks out, they surgeon and others tell me this is the least risky, least invasive type of open-heart surgery you could have. That sounds strange, I know. but here are the details.
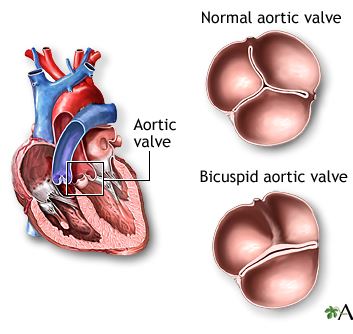
I was born with an abnormal aortic valve. A normal heart valve has three leaves that move together, opening to allow flow and closing to block flow. My aortic valve, however, has only two leaves (cusps is the medics call them). I normally say genetically defective valve, but that’s probably unfair to the valve. It has served me well for 72+ years, but my cardiologist thinks it’s time to replace the two-cusp wonder, and the surgeons who normally do this kind of surgery agree.
The valve has a condition that’s called stenosis, a build-up of calcium (and maybe other stuff) on it. It’s opening and closing fine, and not leaking, but with the degree of buildup on it, it’s only a matter of time until it won’t work properly, or some of the calcium will slough off and cause a problem in my lungs or elsewhere. So the doc says it’s time to replace it, while I’m still “young” and not a very big risk for surgery. Based on tests, they say I’m low risk.
They aren’t saying the valve was the cause of my mini-stroke in January—it most likely wasn’t. But with that health scare, and with their knowledge of how these things go as a man ages, they strongly recommended I have the procedure done now. That was back in mid-February. The surgery will be, most likely, the week of July 22.
Why so long a wait? Well, it isn’t an emergency. My heart is strong. Tests show my arteries are not blocked (“widely patent” is medical speak for a clear artery, and tests show almost all mine are “widely patent”). I have a good ejection fraction, a measure of the squeezing function of the heart. I have no symptoms of heart disease—no angina (thought I did have some last year) and no shortness of breath. Everything is fine except for my genetically defective valve, which is stenotic, calcifies, and perhaps ossified, petrified, and mummified.
With the wonders of modern medicine, most of these valve replacements, maybe 80 percent of them, are done through the groin. That requires one or two days in the hospital and a seven-to-ten-day recovery period. Back in February they thought mine would be done through-the-groin, and they began running the tests needed to know for sure. Well, it turns out that my two-cusp wonder is quite elongated rather than circular. The two manufacturers of the through-the-groin valves cannot guarantee that their valves will fit and lodge properly, with no leakage or looseness.
Hence, they gotta do mine the old-fashioned way. Put me to sleep; switch my breathing to a heart-lung machine; stop my heart; open my chest to expose the heart; detach the aorta; cut out the bad valve; possibly reshape the valve opening; insert and stabilize the new valve; sew me back up; restart the heart; and wake me up. I’ll then have a week or maybe ten days in the hospital, followed by two months of at home recovery. Easy-peasy. Seems almost ridiculous seeing as I have no symptoms. But the tests don’t lie.
One good thing about doing this via open heart is that in ten years, when my replacement valve wears out and I need another valve, presumably I’ll be less strong to withstand another surgery but they will be able to do it through the groin. To every cloud there is a silver lining, even if you have to wait ten years to see it.
But, with every surgery there are risks. What is my heart doesn’t want to re-start when it’s over? What if some calcium decides to slough off during the surgery? What if the anesthesia is at the wrong level? What if my otherwise strong heart is damaged during the surgery?
I’ll have some posts written ahead of time for when I’m in the hospital. Meanwhile, if you’re interested in this kind of condition, you can find quite a few reputable websites that discuss it.
Prayers David for you and Linda. Gary had his replaced the old fashioned way, his was leaking from damaged caused by a. Infection years before. Long story and I won’t bore you with it, he felt so much better after he recovered. His was a titanium valve put in about 30 years ago. His original valve lasted the rest of his life. Only downer was anticoagulants for the duration. I’m sure much has improved in the past 30 years. Prayers for successful surgery, and complete recovery.
Sue: Thanks for reading and commenting. I didn’t know that was one of Gary’s health problems. Many others have gone through what I’m soon to go through.
I appreciate the details! I’ll definitely be praying. I understand what the doctors are saying, about doing the surgery now when you’re younger/healthier. I have a friend (85 today) who badly needs both knees replaced. With her weight and other health issues (diabetic and stage 4 kidney disease), dr’s won’t do surgery due to the risk. So, she’s become basically unable to walk — which has its own issues. I wish I could have foreseen this and urged her to have the knees done even 5 yrs ago. My dad had open-heart surgery about 8 years ago and has done great since! Be aware, as I’m sure you are, that depression following the surgery is really common. Why, I’m not sure. But if you know that going in, it can help you not be surprised and able to cope if it happens. Be good to yourself and I know you’re doing that with looking for good reading material, etc.
Susan: Yes, while I’d rather not undergo such major surgery, it’s better to do it now rather than when the valve deteriorates to the point of giving me problems. Thanks for the caution about depression.
Sorry you’re going through this, Dave. But you’re strong, and God is with you. We’ll be praying. Love you!
Thanks, Katie. And after the surgery (now put off until July 29 or possibly later). When I’m past it, I’ll just be through a fraction of what you’ve experienced.